home


Tony Goovaerts
RN, Nurse Manager of Pre-Dialysis Education Programme, Peritoneal Dialysis and Home HD programme
Cliniques Universitaires St. Luc, Brussels, Belgium
tony.goovaerts@telenet.be

Debbie Fortnum
Editor, EDTNA/ERCA Brand Ambassador Australia/New Zealand
Clinical Nurse Manager Dialysis,
SCGH, Perth, Australia
deborah.fortnum@health.wa.gov.au
8.0 Vascular Access for Home Haemodialysis (HHD)
Introduction
There are three types of vascular access for haemodialysis that can be used at home;
- Arteriovenous fistula (AVF).
- Arteriovenous graft (AVG).
- Central Venous Catheter (CVC) – some restrictions apply.
This section will provide information about how to care for your access at home, how to put in the needles (cannulate) and how to reduce the risk of any problems. It does not talk in detail about surgery for access. It does contain pictures of access and needles.
8.1 Importance of good access
Your blood can only be cleaned well on dialysis if your access works well. A strong/fast blood flow and keeping your access infection free help this. Putting the needles in properly is also important. You may do extra dialysis treatments at home which can increase the risk of problems, but good care of your access can reduce this risk.
- Reducing infection risk: Some dialysis centers will test to see if you have bacteria that can cause infections and treat you if needed. Handwashing must be done perfectly and some centers may recommend the use of gloves.
- Checking for infection and blood flow: You will be taught how to check your access for strong blood flow and signs of infection.
- Keeping to the rules. After training many dialysis centers do regular checks on how you put in the needles and care for your fistula.
8.2 Fistulas and Grafts
8.2.1 Arteriovenous fistula (AVF)
An arteriovenous fistula, simply known as the “fistula” is the most common type of access and has the least problems. Ideally it will be put into your non-dominant hand. It is simply the joining of an artery and a vein. The vein gets larger and this is where the needles go into.
8.2.2 Arteriovenous graft (AVG)
Arteriovenous graft simply known as a “graft” is a good option if you cannot have a regular fistula. They are often put in the upper arm, but sometimes the lower arm or the upper leg. A graft is an artificial tube which is joined between your artery and vein.
8.3 Cannulation (putting in needles)
8.3.1 Importance of self-cannulation (Putting in the needles yourself)
The practice of putting in the needles should be started as soon as possible during training as it is often the part of training people are most worried about.
- By self-cannulating, you will feel in control. You will become an expert of your access.
- If you have problems such as tremor, sight problems, inability to reach puncture sites or even a needle phobia you may need someone else to help with your cannulation at home.
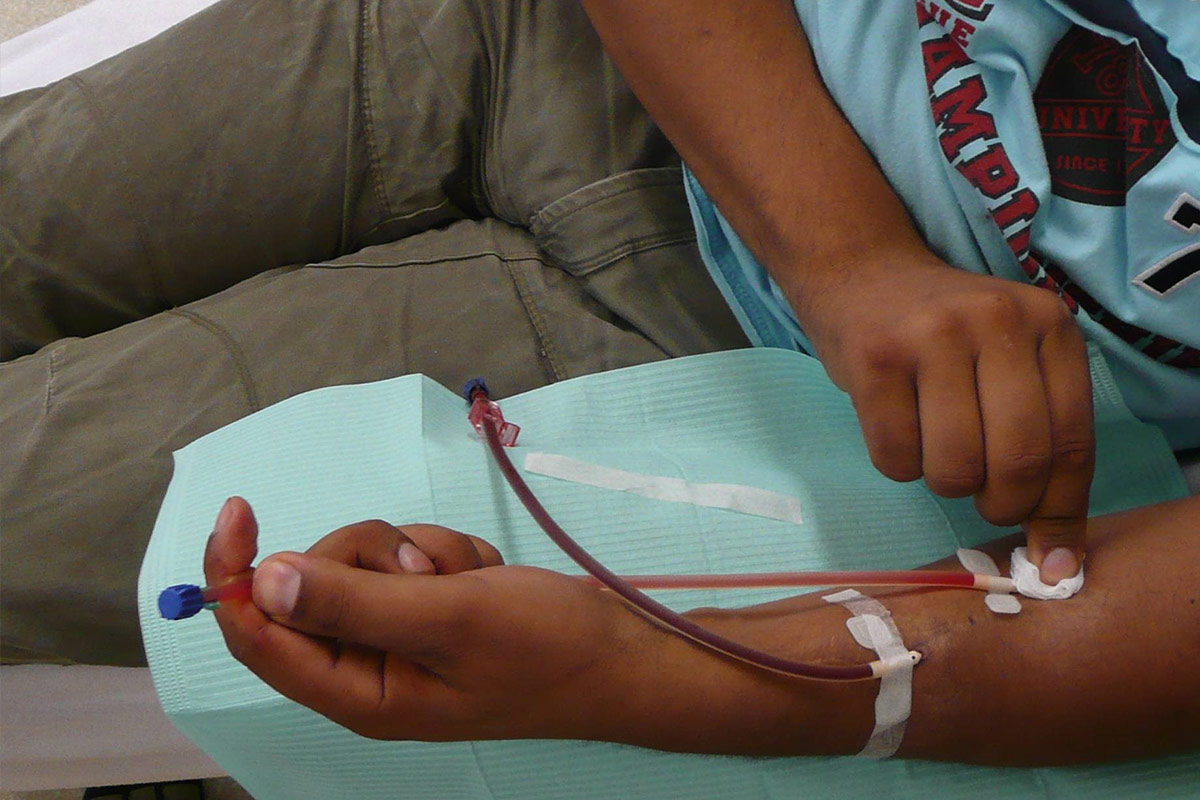
8.3.2 Practical instructions for self-cannulation
You will be taught how to put in the needles. You will also be given all the equipment. Below are some basic steps you will learn.
Preparation
- Cannulate in a clean and draught-free environment with a good light source.
- Do a hand-wash before starting to prepare equipment.
- Prepare equipment such as: disinfectant, drape, sterile dressing pack, tape, syringes, needles, tourniquet, waste bin, sharps container.
- Disinfect hands with an alcohol based rub before aseptic preparation of syringes, needles and tape.
Cannulate
- Wash (scrub) arm.
- Look, feel and listen to the access. Do not cannulate an infected AVF and contact the nurse if you are worried1.
- Disinfect the access with antiseptic.
- Use a tourniquet for an AVF (optional for button-hole cannulation).
- Stabilise the access and insert the needle.
- Tape with one tape first (to avoid accidental pulling out of needle).
- Check for flashback of blood and flush the needle.
Tape securely to prevent infection and the needle falling out.
Removing needle
- Taking the needles out carefully is important. It has to be done at the right angle and once the needle is out mild pressure needs to be applied for a few minutes2.
- When the bleeding has stopped, the sites have to be covered with a small dressing.




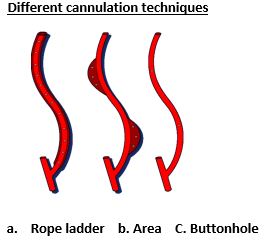
8.3.3 Cannulation techniques (site selection)
It is important to choose carefully where to put the needles. You can either put them;
- In the same spot every time (button-hole).
- Roughly in the same area (area).
…or each time go a little further up or down the fistula (rope-ladder)
The rope ladder technique is a very good cannulation technique and helps the fistula to last longer. Area cannulation has the most problems with thinning of the wall and swellings (aneurysm) formation3,4.
Buttonhole cannulation works well for some patients but the buttonholes have to be carefully established. There can be a higher risk of infection5,6,7.
Your nurses will assess your fistula and work with you to decide the best technique for your fistula.
The recommended technique to put in needles for a graft is the rope ladder technique, (in a line).


8.3.4 Central Venous Catheter (CVC)
General information
A Central Venous Catheter (CVC) is usually a temporary access. In some countries, the use of CVC is not allowed in the home setting. Many countries insist on a second person to help with the CVC but not all. There is a higher risk of infection (on the skin or inside the body) compared to fistulas and grafts. They also block up more easily due to small blood clots.
There are different types of CVC and different types of caps. Each dialysis unit will have its own way of looking after the CVC and will teach you:
- How to do the dressing where it goes into the skin.
- If you can shower and if so how to do this.
- How to check for signs of infection.
- How to keep the CVC secure and in place.
- When, where and how to change the caps.
8.3.5 Practical instructions for successful CVC handling
- Proper hand washing (with liquid soap) is mandatory before starting.
- Disinfect hands with an alcohol based rub.
- Wearing mask is usually advised (you and your and carer).
- Whatever disinfectant agent is used, leave it on for the right amount of time.
- Avoid pulling on the CVC. During treatment lines have to be secured.
Keep the lines clamped between dialysis and check regularly that the caps are screwed on tight.
8.3.6 Preventing a blood clot in the CVC
After each dialysis treatment the CVC is flushed and then special drugs such as heparin are put into the CVC to make sure it doesn’t ‘clot’.



Conclusion
All types of vascular access can be used in the home setting. A well-functioning vascular access is a key success factor for home dialysis. Care of the access is a very important part of the training programme. It is important to follow the instructions you are given.
Retraining, observation of the technique during home visits is common and will help reduce your risk of infection and how long your access lasts.
Useful websites:
This site has lots of information about dialysis. This is the direct link to the page about access for dialysis http://www.kidneypatientguide.org.uk/access.php
References
- Sousa CN, Apostolo JL, Figueiredo MH, Martins MM, Dias VF. Physical examination: how to examine the arm with arteriovenous fistula ; Hemodial Int. 2013; 17:300-306.
- NKF/KDOQI Updates Clinical Practice Guidelines and Recommendations. Clinical Practice Guidelines on vascular access (2006; cited 2012 Dec 9).
- Verhallen AM, Kooistra MP, van Jaarsveld BC. Cannulation in Haemodialysis: Rope-ladder or buttonhole technique? Nephrol Dial Transplant 2007; 22:2601-2604.
- UK Renal Association (2008-2011) Clinical Practice Guidelines. Vascular Access for Hemodialysis. Complications of vascular access(Guidelines 6.1-6.4) 5th edition 26b
- MacRae JM, Ahmed SB, Atkar R, Hemmelgarn BR. A randomized trial comparing buttonhole with rope ladder needling in conventional haemodialysis patients. Clin J Am Soc Nephrol 2012;8(3):1632-1638.
- Labriola L, Crott R, Desmet C, Andre G, JAdoul M. Infectious complications following conversion to buttonhole cannulation of native arteriovenous fistulas : a quality improvement report. Am J Kidney Dis 2011;57(3):442-8.
- Nesrallah GE, Cuerden M, Wong JH, PierratosA. Staphylococcus aureus bacteremia and buttonhole cannulation: long term safety and efficacy of mupirocin prophylaxis. Clin J Am Soc Nephrol 2010;5(6):1047-53.
EDTNA/ERCA Secretariat
Uzubaliu 7, Miklusenai, Alytaus r. sav. 62466
Lithuania
E-mail: secretariat@edtnaerca.org
E-mail: secretariat@edtnaerca.org
Www:
www.edtnaerca.org
Head Office
EDTNA/ERCA, Seestrasse 91, CH 6052 Hergiswil, Switzerland



