
Ways of nutritional support
Dietary counselling (Ikizler et al., 2020)
Patients should be encouraged to increase his/her nutritional intake by:
- Modifying and/or liberate diet according to individualized needs
- Providing small frequent meals and low potassium and phosphate energy dense snacks
- In case or early satiety, patients should be advised to consume protein foods first if they are on dialysis. As those not on dialysis tend to need less protein, it is important that dietary advice in this situation doesn’t encourage high levels of protein.
- Patients should be advised to choose energy dense/ low volume dietary choices.
Food Fortification
In case of more profound malnutrition food fortification can be used to increase energy and protein intake. Fortification is the addition of nutrients to common foods to increase energy and protein intake.(Ikizler et al., 2020)
Energy fortification can be established with the addition of fat and carbohydrates in the food. Common ways of achieving that is the addition of:
- olive oil, vegetable oils, margarine, butter
- sugar and honey in absence of diabetes mellitus
- specific products that provide energy by fat and carbohydrates.
Protein fortification can be achieved with the addition of:
- eggs and cream cheese
- commercially available protein powers or liquid protein supplements mainly from casein or collagen
ONS
If nutritional counseling alone fails to improve nutritional status, Oral nutritional supplements (ONS) can be used. (Fiaccadori et al., 2021)
Oral Nutritional supplements for CKD patients are usually:
- energy dense, providing >1.5 Kcal/ ml to avoid fluid overload
- low in potassium, sodium and phosphate whilst containing micronutrients
They can cover the needs of patients who are able to cover 20 Kcal/kg/day per day and 0.8g/kg/day from spontaneous energy and protein intake respectively.
IDPN
In stable undernourished maintenance haemodialysis patients with low compliance or tolerance to ONS can have intradialytic parenteral nutrition (IDPN) considered (Chan, 2021)
Intradialytic parenteral nutrition is:
- a cyclic parenteral nutrition (PN) provided during haemodialysis through the venous way of the dialysis line, three times per week.
- It provides 15-20 Kcal/kg (800-1200 Kcal in total) and 0.5-1g/ kg protein (30-60 g/session) per HD session, in the form of fat, carbohydrate and protein
- It equals to the nutritional support of 400-600 Kcal /day. (Sabatino et al., 2014)
- If not supplemented with micronutrients, it doesn’t contain any vitamins or minerals therefore is not a whole source of nutrition
IDPN is administered via an infusion pump that can overcome venous pressure in the dialysis blood lines. This fluid is then mixed with the patient’s venous blood and returned to the body through the venous access. During IDPN, up to 1lt of parenteral nutrition can be administered at a maximum rate of 250 ml/h, to be able to infuse 1lt in 4 hours.(Carrero et al., 2023)
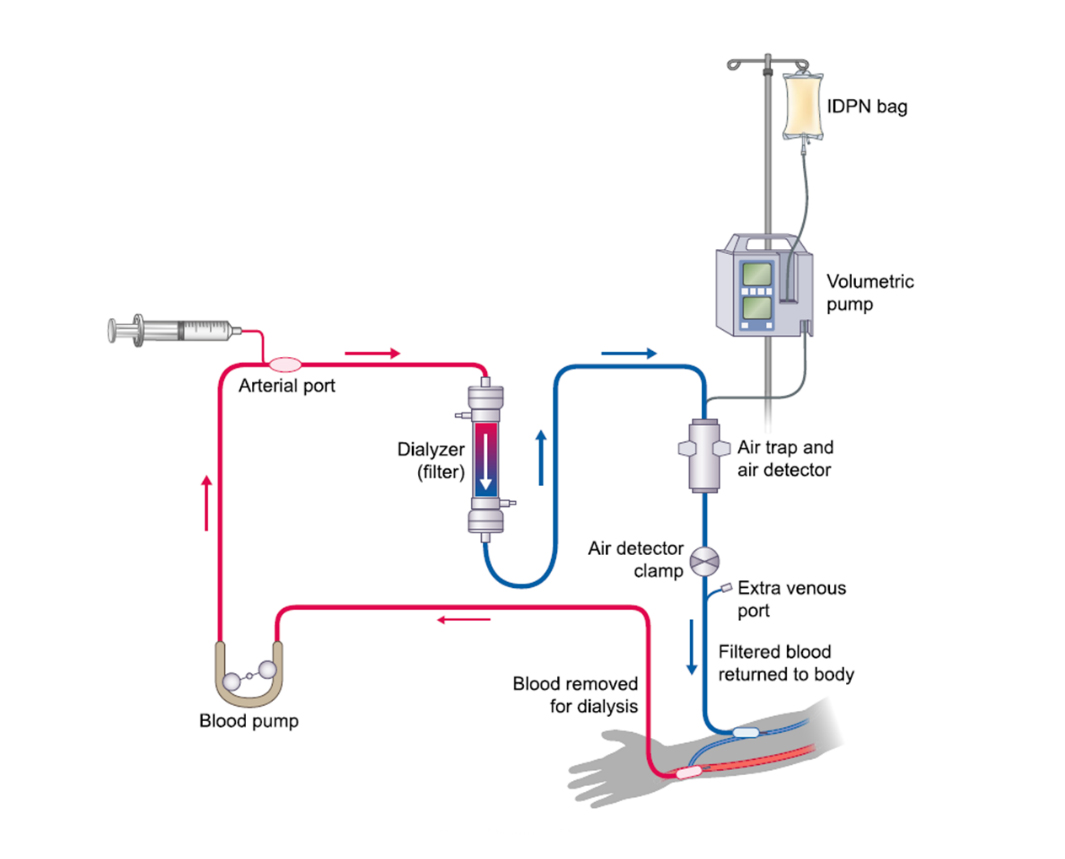
Schematic review of hemodialysis circuit. Adapted from: National Institute of Diabetes and Digestive and Kidney Diseases, https://www.niddk.nih.gov/health-information/kidney-disease/kidney-failure/hemodialysis
IPN
In case of malnourished patients on peritoneal dialysis, intraperitoneal nutrition (IPN) can be used.
IPN is a non-invasive nutrition support therapy for patients on PD. It contains amino acids needed for supplemental nutrition support and it is recommended for patients who are unable to meet nutrient needs through oral diet and traditional means of protein repletion
IPN is administered in the same method as the peritoneal dialysis (PD) exchanges by replacing one of the daily PD exchanges. It contains amino acids and (not always) dextrose and it can cover up to 25% of the daily protein needs.(Tjiong et al., 2008)
Full nutritional Support
Enteral nutrition by tube feeding (TF) is the provision of nutrients by feeding tube and should be a choice for patients with low levels of consciousness or patients with dysphagia, to avoid the risk of aspiration. In patients with gastroparesis, Naso jejunal TF should be chosen to facilitate better promotion of food in the gut and in patients requiring long periods of enteral nutrition, percutaneous endoscopic gastrostomy or jejunostomy (PEG or PEJ) should be considered.(Fiaccadori et al., 2021)
EDTNA/ERCA Secretariat
Uzubaliu 7, Miklusenai, Alytaus r. sav. 62466
Lithuania
E-mail: secretariat@edtnaerca.org
E-mail: secretariat@edtnaerca.org
Www:
www.edtnaerca.org
Head Office
EDTNA/ERCA, Seestrasse 91, CH 6052 Hergiswil, Switzerland



